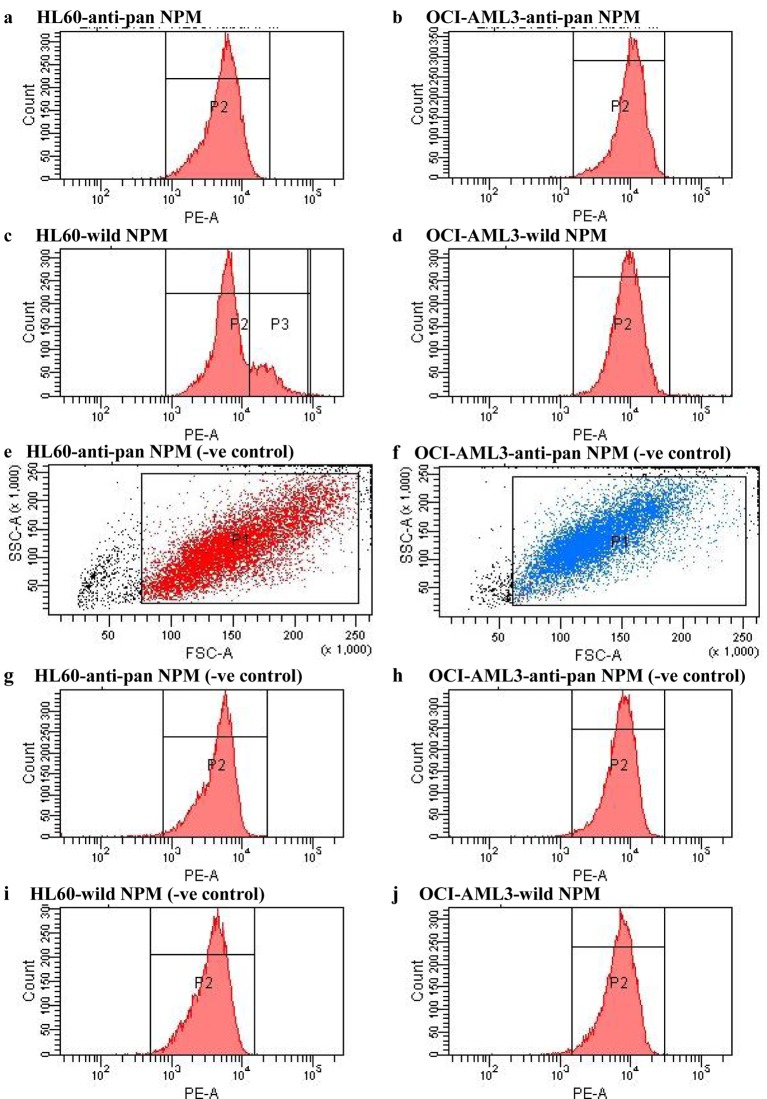
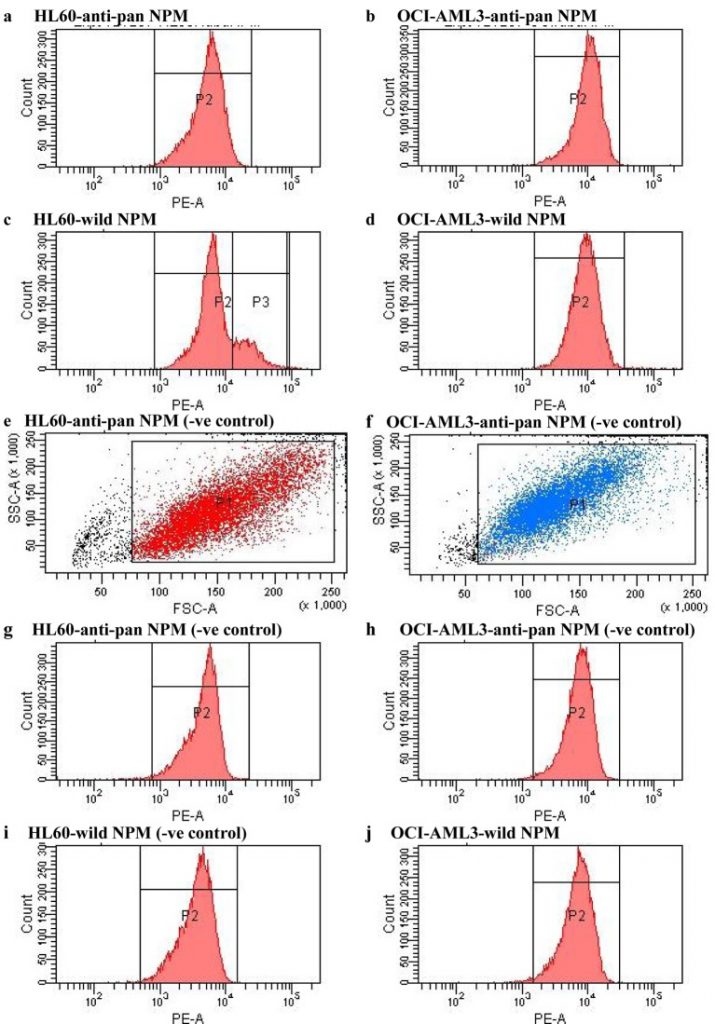
In our earlier work, we provided sturdy proof that nucleophosmin (NPM) gene mutation has an very important place in leukemogenesis of main acute myeloid leukemia (AML). Furthermore, we speculated a model new centered treatment in victims with main AML and bearing mutated NPM (mNPM).
Based on these outcomes together with findings of completely different researchers, it was necessary to develop a way for proper detection of mNPM. Our methodology based on utilizing the most recent transfer cytometeric strategies and gadgets in measuring mNPM. Attributed to their availability and technical feasibility, we used human leukemia cell traces to validate our methodology.
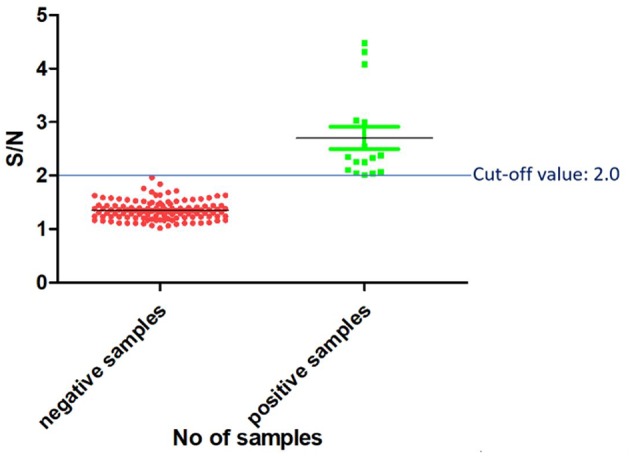
The necessary findings had been differential expression of wild-type NPM (wtNPM) all through the same sample. Furthermore transfer cytometry (FCM) was a straightforward straightforward instrument for quantitative assay of mNPM.
In this work we developed an trendy method that may enable quantitative assay of mNPM, and ease its use as a biomarker in cytogenetic and molecular prognostication of main AML. In addition the look at immediate that FCM would possibly differentiate mNPM expression inside cells of the similar affected particular person thus could be used for monitoring of minimal residual sickness.
Quantitative Assay of Mutated Nucleophosmin in Acute Myeloid Leukemia.
Accuracy of a reverse dot blot hybridization assay for simultaneous detection of the resistance of Four anti-tuberculosis medication in Mycobacterium tuberculosis isolated from China.
Drug resistant tuberculosis poses a tremendous downside for tuberculosis administration worldwide. Timely dedication of drug resistance and environment friendly explicit particular person remedy are necessary for blocking the transmission of drug resistant Mycobacterium tuberculosis. We aimed to find out and think about the accuracy of a reverse dot blot hybridization (RDBH) assay to concurrently detect the resistance of Four anti-tuberculosis medication in M. tuberculosis isolated in China.
In this look at, we utilized a RDBH assay to concurrently detect the resistance of rifampicin (RIF), isoniazid (INH), streptomycin (SM) and ethambutol (EMB) in 320 medical M. tuberculosis isolates and in distinction the outcomes to that from phenotypic drug susceptibility testing (DST) and sequencing.
The RDBH assay was designed to verify as a lot as 42 samples at a time. Pearson’s chi-square check out was used to compute the statistical measures of the RDBH assay using the phenotypic DST or sequencing as a result of the gold commonplace methodology, and Kappa id check out was used to seek out out the consistency between the RDBH assay and the phenotypic DST or sequencing.
The outcomes confirmed that the concordances between phenotypic DST and RDBH assay had been 95% for RIF, 92.8% for INH, 84.7% for SM, 77.2% for EMB and the concordances between sequencing and RDBH assay had been 97.8% for RIF, 98.8% for INH, 99.1% for SM, 93.4% for EMB.
Compared to the phenotypic DST outcomes, the sensitivity and specificity of the RDBH assay for resistance detection had been 92.Four and 98.5% for RIF, 90.Three and 97.3% for INH, 77.Four and 91.5% for SM, 61.Four and 85.7% for EMB, respectively; in comparability with sequencing, the sensitivity and specificity of the RDBH assay had been 97.7 and 97.9% for RIF, 97.9 and 100.0% for INH, 97.Eight and 100.0% for SM, 82.6 and 99.1% for EMB, respectively.
The turnaround time of the RDBH assay was 7 h for testing 42 samples.Our information immediate that the RDBH assay would possibly perform a speedy and atmosphere pleasant methodology for testing the resistance of M. tuberculosis in the direction of RIF, INH, SM and EMB, enabling early administration of acceptable remedy regimens to the affected drug resistant tuberculosis victims.
Peste des petits ruminant (PPR) is an economically vital extreme viral illness of small ruminants that impacts primarily the respiratory and digestive tract. Specific detection of the PPR virus (PPRV) antigen performs an vital function in the illness management and eradication program.
In this research, an oblique enzyme-linked immunosorbent assay (ELISA) based mostly on the recombinant goat signaling lymphocyte activation molecule (SLAM) as the seize ligand was efficiently developed for the detection of the PPRV antigen (PPRV SLAM-iELISA).
The assay was extremely particular for PPRV with no cross-reactions amongst foot and mouth illness virus, Orf virus, sheep pox virus, and goat pox virus and had a sensitivity with a detection restrict of 1.56 × 101 TCID50/response (50 μl).
Assessment of 136 samples confirmed that the developed PPRV SLAM-iELISA was properly correlated with real-time RT-qPCR assays and commercially accessible sandwich ELISA for detection of PPRV and confirmed relative sensitivity and specificity of 93.75 and 100.83%, respectively.
These outcomes counsel that the developed PPRV SLAM-iELISA is appropriate for particular detection of the PPRV antigen. This research demonstrated for the first time that the goat SLAM, the mobile receptor for PPRV, can be utilized for the growth of a diagnostic methodology for the detection of PPRV.
Development of an Enzyme-Linked Immunosorbent Assay Based on CD150/SLAM for the Detection of Peste des Petits Ruminant Virus.
Global coagulation assays in transgender girls on oral and transdermal estradiol remedy.
The thrombotic results of estradiol remedy in transgender girls are unclear. Global coagulation assays (GCA) could also be higher measures of hemostatic operate in comparison with customary coagulation checks.To assess the GCA profiles of transgender girls compared to cisgender controls and to check how GCA differ between routes of estradiol remedy in transgender girls.
Cross-sectional case-control research.General neighborhood.Transgender girls, cisgender male and cisgender feminine controls.
Citrated blood samples had been analyzed for (i) complete blood thromboelastography (TEG®5000), (ii) platelet-poor plasma thrombin technology (calibrated automated thrombogram); and (iii) platelet-poor plasma fibrin technology (general hemostatic potential assay). Mean distinction (95% confidence intervals) between teams are introduced.
Twenty-six transgender girls (16 oral estradiol, 10 transdermal estradiol) had been in comparison with 98 cisgender girls and 55 cisgender males.
There had been no variations in serum estradiol focus (p=0.929) and length of remedy (p=0.496) between formulations.
Transgender girls demonstrated hypercoagulable parameters on each thromboelastography (most amplitude +6.94mm (3.55, 10.33), p<0.001) and thrombin technology (endogenous thrombin potential +192.62nM.min (38.33, 326.91), p=0.009; peak thrombin +38.10nM (2.27, 73.94), p=0.034) however had elevated general fibrinolytic potential (+4.89% (0.52, 9.25), p=0.024) in comparison with cisgender males.
No vital adjustments had been noticed relative to cisgender girls. Route of estradiol supply or length of use didn’t affect the GCA parameters.Transgender girls on estradiol remedy demonstrated hypercoagulable GCA parameters in comparison with cisgender males with a shift in the direction of cisgender feminine parameters. Route of estradiol supply didn’t affect the GCA parameters.
How do tests that reveal the SARS-CoV-2 virus work?
Covid-19
diagnostic tests are an essential tool for monitoring the spread of the
pandemic. The World Health Organization (WHO) has repeatedly asked health
agencies to make coronavirus testing a top priority, but international response
has been mixed.
Why does their use vary so much from one country to another?
Thanks to a
combination of enabling regulations and logistical readiness, some countries,
such as South Korea and Singapore, have been able to rapidly deploy massive
test campaigns targeting thousands of individuals; but elsewhere, several
countries have struggled to keep pace.
What are the new types of tests in preparation?
Meanwhile, in the
United States, faced with delays of several weeks from hospitals and
manufacturers, university research laboratories have developed their diagnostic
tools to meet needs.
Test, instructions for use
Most Covid-19
tests are now performed on viral genetic material from samples from the nose or
pharynx. They are based on a molecular biology tool designated by the acronym
RT-PCR. PCR (for polymerase chain reaction) is a method of duplicating (or
amplifying) a DNA sequence in very large numbers thanks to an enzyme, the polymerase.
We can then analyze the DNA.
However, since
the coronavirus genome is in the form of RNA, it must first be transformed into
DNA, which another enzyme does, reverse transcriptase (RT).
Amplification
starts from short sequences, added primers, complementary to the sequence to be
duplicated. However, PCR can only detect the virus when it is present, and is
of no use when the epidemic is resolved. What is more, it sometimes produces
false positives when the reagents (in particular the primers and the products
necessary for the duplication of DNA) are contaminated.
Laboratories
around the world quickly adapted their RT-PCR tests to SARS-CoV-2, by designing
appropriate primers, complementary to various fragments of the genetic sequence
of the virus.
Which countries have been reactive?
Several countries
have been able to test very large numbers of people (see figure below). South
Korea reacted when the first cases appeared at the end of January by deploying
large quantities of rapid tests and then monitoring those in contact with those
who had tested positive. Regulations promulgated after the Middle East
respiratory syndrome (MERS) epidemic in 2015 (with 186 cases and 35 deaths,
South Korea was the second most affected country after Saudi Arabia which counted
688 cases and 282 deaths) allowed rapid release of a version of the WHO test,
and four companies produced enough to test up to 10,000 people per day.
In this way,
explains Angela Rasmussen of Columbia University in New York, the South Korean
authorities were able to identify the slightly ill and asymptomatic people and
prevent them from spreading the virus. “The country has not had to take the
drastic social distancing measures as in other countries,” she added.
As for Singapore,
the city-state developed a test as soon as the coronavirus appeared in China,
explains Vernon Lee, of the Singapore Ministry of Health, and was very early in
battle order to track down the cases. Hospital laboratories were quickly given
the green light to use other authorized PCR tests, provided that the results of
the first cohort were validated by a national laboratory. They also focused the
tests on the most essential cases such as patients with pneumonia or people at
high risk, for example elderly people.
College of public health and occupational physicians -Singapore-
Essential logistics
were installed after the appearance in 2003 of another coronavirus, the
SARS-Cov: it notably provides sufficient capacities in laboratories, trained
personnel, reagents…
“In Singapore, we are ready and have ” a medical and hospital system strengthened since the SARS episode. It’s not something we created because of the Covid-19, ”
Vernon Lee.
The latecomers
Health experts
have criticized the United States for its slow response to the pandemic, in
particular the low availability of tests and their slow implementation.
According to specialists, these failures allowed the virus to spread without
being detected and imposed strict social distancing measures to contain it.
US health
officials have admitted their fault. At a congressional hearing on March 12, the
director of the National Institute of Allergies and Infectious Diseases
(NIAID), Anthony Fauci, said that the country “is unable” to test the
population and was not in able to meet demand for testing.
Kenneth Bernard,
a former adviser to several US presidents on biodefense, said a coordinator or
a White House office responsible for responding to the pandemic could have
facilitated communication between the agencies and drawn up a plan to intensify
the tests. But the person who held the office left President Donald Trump’s
National Security Council … in May 2018.
“We had a problem
with the scale. It is one thing to do a benchmark test at the CDC (Center for
Disease Control and Prevention), but another to do millions of them, “warns
Kenneth Bernard.
Rigid regulations
for new diagnostic tests have been an additional barrier. Initially, the only
approved American test was created by the CDC, but it was found to be
defective. And only public health services were allowed to use it. The Food and
Drug Administration (FDA) did not relax these rules until the end of February
and did not allow private labs to test until mid-March. It was only on the 21st
that the US authorities authorized a rapid test that did not require samples to
be sent to a laboratory. It should be ready soon.
With the federal
response long overdue, the virology laboratories at the University of
Washington in Seattle organized the first major national testing operation. The
researchers adapted the WHO protocol to work with the reagents and platforms
they had on hand. Dozens of other laboratories and research consortia have
followed suit.
“The federal
government made the decision to severely limit access [to the tests] at first,”
said Joshua Sharfstein, a former FDA official. “If you could go back and tell
the FDA in mid-January that you’re really going to need a million tests soon
enough, they would have chosen a different strategy. “
What about serological tests?
One of the main
goals is to develop a serological test, which is one that can detect past viral
infections by looking for antibodies that a formerly infected person has
produced to fight the virus. Such a test would reveal the extent of viral
spread in a population and would provide useful public health information.
“For the moment,
it is clear that we are only seeing the tip of the iceberg: patients so
severely affected that they must be hospitalized or even receive intensive care
there,” explains Robert Garry, virologist at Tulane University, in New Orleans,
Louisiana. “What is worrying is that there are a lot of patients with little or
even asymptomatic disease outside. “
Several groups,
including that of Robert Garry, are working on carrying out such a serological
test. Another team, including researchers from Icahn School of Medicine at
Mount Sinai Hospital in New York, developed one that she describes in a
prepublication, not peer reviewed, posted on medRxiv on March 18. “We don’t see
any obstacle to carrying out these tests, only a few adjustments,” says Robert
Garry.
A team in
Singapore used serological tests to trace contacts of patients, but at the
time, the method used had not been validated for clinical use. “We think this
is the first time in the world that this type of testing has been used in this
context,” said Danielle Anderson, virologist at the faculty of medicine at Duke
and Singapore Universities, in Singapore, during a press conference in
February.
Make way for innovation
Research groups
led by two of CRISPR’s leading specialists, the tool that makes it easy to modify
an organism’s genome, are each working on tests that leverage this gene editing
technique to improve testing.
First, at the
University of Washington, virologist Keith Jerome and his colleagues improved
the SHERLOCK test (for specific high sensitivity enzymatic reporter unlocking)
developed by Feng Zhang at the Massachusetts Institute of Technology. The
latter said he had sent some 1,600 test kits to ten laboratories around the
world.
Next, Mammoth
Biosciences, a California-based biotechnology company co-founded by Jennifer
Doudna of the University of California at Berkeley, is working on another
CRISPR-based method called DETECTR to detect SARS-CoV-2.
Both techniques
use CRISPR’s ability to recognize and cut specific genetic sequences. Here, he
also cuts a reporter molecule added to the reaction, which relatively quickly
reveals the presence of viral genetic material.
“Whenever we are
faced with an epidemic, we are late because we do not have rapid diagnostic
tools to detect and identify the new organism in question,” said Charles Chiu
of the University of California at San Francisco, who works with Mammoth
Biosciences. “The main advantages of CRISPR are its specificity and speed, a
test which can be carried out in 5 to 10 minutes. “
Robert Garry, at Tulane, is optimistic about such
advances. “It is a powerful technique. I’ve seen it work with the Zika virus
and a few other viruses, “he says. “If anyone can find a way to lessen the
impact of the Covid-19, let’s do it. “